Hearing Wrap Up: Physicians and Patients Need Improved, Effective, Up to Date Vaccine Safety Systems
WASHINGTON — The Select Subcommittee on the Coronavirus Pandemic held a hearing titled “Assessing America’s Vaccine Safety Systems, Part 2” to further examine vaccine safety reporting and injury compensation systems. Today’s hearing uncovered substantial evidence that inadequate vaccine safety systems jeopardized the safety and health of Americans during the COVID-19 pandemic. Witnesses testified to personal experience reporting vaccine injuries that were not recognized by the federal government and described the legal ramifications of flooding an overwhelmed system with vaccine injury claims. Select Subcommittee Members pointed out serious shortcomings in America’s vaccine injury reporting and compensation systems that caused fractures in the doctor-patient relationship. It is clear that healthy Americans were coerced into compliance with unscientific vaccine mandates without a sufficient system in place to monitor injuries or compensate injured individuals. The Select Subcommittee is committed to ensuring that vaccine safety systems are improved, effective, and up to date prior to the emergence of a future public health crisis.
Key Takeaways
America’s vaccine safety systems often failed to accurately identify injuries or follow-up on serious reports made by physicians during the COVID-19 pandemic. Reform is necessary to correct these failures.
- Dr. David Gortler — former senior executive leader at the Food and Drug Administration (FDA) — detailed why America’s vaccine injury reporting systems are not structured in a way that allows physicians to easily and accurately report adverse events: “No, they aren’t and I can explain why. I don’t think the collection systems are adequate for the following reasons. As a physician, you’ll know, and there’s other physicians in here, a normal physician visit is usually billed out as a code…a 99213 pays a physician something like $75 to be able to, you know, interview, assess, diagnose, and prescribe. And if a patient were to report an adverse event during one of those events, a physician wouldn’t really have time to collect it and go on the phone and spend an hour with the FDA MedWatch system. Likewise, a pharmacist is also someone who receives quite a bit of safety complaints, but a poor pharmacist, you know, working behind the counter at one of these grueling chain pharmacies, they have metrics by their employer and their metrics are to hammer as many round pegs in a round hole as fast as they can…There’s no way to reimburse for them to be able to report adverse events. And so, because of that, there was a study funded by the AHRQ that came through out of Harvard, that found that it’s only the very, very low digits, the single like 1%, the very, very low single digits of adverse events ever reported to VAERS. And I think there needs to be a better collection method. There needs to be more vigilance about reporting by health care professionals.”
- Select Subcommittee Minority Member Kweisi Mfume (D-Md.) described serious shortcomings in America’s vaccine injury compensation systems that present legal complications and do not adequately serve the vaccine injured: “Victims concern me. And being able to find a way to get compensation is important…I can tell you that people who don’t have a voice, who were somehow or another injured by the vaccine and unable to get injury compensation, just concerns me, and I hope it concerns all of us. The VICP shortage of masters tells me that things don’t move through the courts as they should for many of them. The litigation back up concerns me because it’s only probably going to get worse unless we put resources to it. It’s kind of like what Dr. Whelan said about the systems that are in place. They probably were meant well, but we didn’t do the right thing to resource them.”
Dr. Whelan testified that the FDA refuses to acknowledge the death of a young boy who died shortly after receiving his second COVID-19 vaccination. This raises serious questions about other discrepancies in our vaccine safety systems.
- Dr. Patrick Whelan — an Associate Clinical Professor of Pediatrics in the UCLA Division of Rheumatology — detailed a specific example of the Department of Health and Human Services’ Vaccine Adverse Event Reporting System (VAERS) failing to provide Americans with accurate data about vaccine injuries: “At a personal level, I had the experience of caring for a young child who suffered a cardiac arrest shortly after receiving his second COVID vaccination. I filed a VAERS report to bring his plight to the attention of our colleagues at the FDA while he was being kept alive in our pediatric intensive care unit. A week later, after this young man expired as a result of the anoxic injury to his brain, I attempted to update the VAERS system to reflect this more tragic outcome but discovered that the system was not set up to acknowledge a change in outcomes like this. I brought the case directly to the attention of Dr. Marks, and was able to meet ultimately about a month later with staff members at the FDA. But even now, the VAERS System indicates that this boy’s injury was cardiac arrest and gives no clue to the ultimate outcome.”
The sanctity of the doctor-patient relationship needs to be restored in order to increase public trust in our federal health agencies following the COVID-19 pandemic.
- Minority witness Dr. Yvonne Maldonado — Chief of the Division of Infectious Diseases in the Department of Pediatrics at Standford University School of Medicine — agreed with Chairman Wenstrup that patients and doctors should always have the opportunity to discuss the risks associated with receiving the COVID-19 vaccine: “Absolutely. I believe that the bond between a physician and a parent and a patient is sacred and really should be a transparent discussion.”
- Rep. John Joyce (R-Pa.) — a retired physician who treated patients for over 25 years — spoke to the importance of restoring public trust in vaccine safety systems by ensuring physician autonomy: “The doctor-patient relationship needs to be re-emphasized as we discuss how to restore public confidence in vaccines. To accomplish this, we must seriously examine the failures of our vaccine safety system and reform these systems to better support patients and to better support doctors. Doctors must have the most up to date information on any potential vaccine side effects in order to appropriately counsel patients. Our current vaccine safety mechanisms are insufficient to accomplish this goal, and patients ultimately suffer the consequences.
Member Highlights
Select Subcommittee on the Coronavirus Pandemic Chairman Brad Wenstrup (R-Ohio), D.P.M, revealed a severe loss of public trust in America’s federal health agencies that was created by a lackluster vaccine safety system that did not prioritize transparency.

Chairman Wenstrup: “Dr. Whelan, do you believe that it’s appropriate to house all of the potential updates and corrections to VAERS on a nonpublic database?”
Dr. Whelan: “I think that there is a lot of trust involved in the medical community, but also for the general public, that something is happening behind the scenes when you can’t see it right out in front. And I think too, that people were very aware that you didn’t have the kind of follow up on vaccination, generally, that we expect, for instance, from our pediatricians, where you’ve got a nurse who’s going to call the following week and make sure that your child is doing okay. And I mean, my own strong feeling is that we really needed a much more proactive surveillance mechanism.
“You have to have some level, I think, of internal dialog that takes place. But I think ultimately, as you alluded to earlier, you have to be able to create some level of trust among people. And I think the system currently does not cultivate that.”
Rep. Debbie Lesko (R-Ariz.) detailed a failure in the federally regulated vaccine safety systems by highlighting a constituent who was faced with a vaccine injury and never received recognition or compensation.
Rep. Lesko: “I’m glad to hear that we actually may have bipartisan support in helping the victims because the system is obviously broken. And I just want to emphasize that by saying what happened to my office. So as of January 1st of 2024, this year, the total number of CICP COVID claims filed was 12,854. I have a constituent that had a very severe reaction to the COVID vaccine. He filed a claim. He hasn’t heard anything. He hasn’t heard anything back. So my staff, who’s sitting in the back, called and contacted the CICP legislative affairs person and said, okay, what’s the update on this person? They couldn’t give him any update. The he asked, how many of the claims have you processed, have you done? And the answer was, we don’t have that information. I mean, how can you not have that information? This is absolutely ridiculous. And, Mr. Chairman, I think this is a really big problem. They don’t even have the information of how many claims they’ve processed or they’ve awarded. I mean, it was $41,000, I believe has been awarded in the CICP. And, you know, with how many claims? 12,854 claims, I mean, that’s like nothing.”
Rep. Nicole Malliotakis (R-N.Y.) discussed shortcomings in America’s vaccine safety systems that created confusion, failed to properly inform the American public about vaccine injuries, and deteriorated public trust in vaccine safety during the COVID-19 pandemic.

Rep. Malliotakis: “In your expert opinion, what are the most critical weaknesses in the government’s vaccine safety surveillance systems? What specific steps could the FDA take to reduce reliance on manufacturers and increase transparency to strike a balance between promoting vaccine confidence while allowing space for addressing legitimate concerns openly?”
Dr. Gortler: “So the one-word answer is transparency. Period. But it’s not clear to me, you know, when the FDA — the FDA, is imperfect and when they do things that are a little bit shortcoming, I don’t have a problem, you know, speaking up and saying something about it. But when you look at the lack of information, both in the label and the technical documentation of how it’s manufactured, how mRNA shots in particular are evaluated for safety, there’s just too much information missing.”
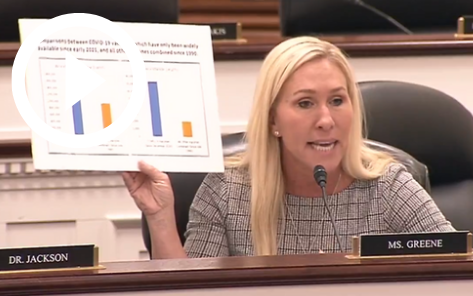
Rep. Marjorie Taylor Greene (R-Ga.) highlighted how healthy Americans were coerced into compliance with unscientific vaccine mandates without a sufficient system in place to monitor injuries or compensate individuals harmed by the mandates.
Rep. Greene: “Nothing creates vaccine hesitancy like ignoring people when they’re reporting problems with vaccines that they’re being mandated and forced to take. Vaccines that they have to take in order to keep their job. Vaccines that they have to take in order to be able to go to restaurants, go into stores, go into public places. Vaccines the doctors are telling them to take, but yet when they’re screaming from the rooftops, something’s wrong with the vaccines, I’m telling you, that creates vaccine hesitancy.
“The other problem is, is when you get censored on the internet, or you get permanently banned on social media when you were a victim of a vaccine injury or a doctor trying to report what you were seeing in your patients from vaccines. This chart right here, this represents vaccine reports from all vaccines since 1990. 34 years. This represents reports on the COVID-19 vaccines since December of 2020, less than four years. Something’s wrong with the vaccines. And just because people are walking around, and they’ve been vaccinated, and they’re not reporting a problem, doesn’t mean other people aren’t having problems. And this has been virtually ignored, so much so, not only has it been ignored, it’s also been censored and banned and labeled misinformation.”
Rep. John Joyce (R-Pa.), M.D., emphasized the importance of preserving the doctor-patient relationship in times of medical crisis to ensure open communication surrounding vaccines and vaccinating children.

Rep. Joyce: “Can you speak about the benefits of ongoing and effective communications for physicians on the front line and those who are responsible for providing health care guidelines?”
Dr. Whelan: “I run a center at UCLA dealing with children who have neuroimmune problems, so I see a lot of kids that have autism and OCD and tic disorders. And so, I’m confronted constantly with this question, you know, should my child be vaccinated? And I also have a lot of kids in our practice who have not been vaccinated at all. So, it’s really an interesting balancing act because on the one hand, I want to be sensitive to the concerns that these families have. I also want to express sensitivity to the fact that we really don’t know a lot about where autism comes from.
“You have to be able to communicate to people that things like measles have the capacity to permanently damage the immune system of that child and could potentially kill them.”
###